Epicrisis on the use of LCD
Child B 11 years old was in the department of thoracic surgery with 30. 03.21. by 20.09.21. diagnosed with:
| CLINICAL DIAGNOSIS: | |
| Principal: | Gastroesophageal reflux. Adhesive intestinal obstruction in the outcome of repeated surgical interventions. Operation 06.04.2021: Relaparotomy, viscerolysis, fundoplication, resection of the jejunum, imposition of interintestinal anastomosis |
| Complications: | Multiple perforations of the small intestine. Fecal peritonitis. Operation 08.04.2021: Relaparotomy, resection of the jejunum, enterostomy. Sepsis. Septic shock. SPON ( Respiratory, heart failure, acute renal damage, hepatic insufficiency)Abscess in the right lateral canal and pelvis. S-m cholestasis. Thrombosis of the external and common iliac veins on the right with spread to the inferior vena cava. Polyserosite: hydrothorax on both sides, hydropericardium. Operation13.04.2021: Relaparotomy. Rehabilitation of the abdominal cavity. Procedure CVVH 08.04.2021 -09.04.2021; 10-12.04.2021; 13-14.04.2021 Sytosorb 08.04.2021; 10-11.04.2021; 13-14.04.2021. Divergence of postoperative sutures. Necrosis of the skin of the anterior abdominal wall. Operation 20.04.2021: necrectomy. Operation 22.04.2021: necrectomy; suturing of intestinal fistulas, installation Vacuum. Pneumonia on the right |
| Concomitant | Relaxation of the right dome of the diaphragm. Funnel-shaped deformity of the chest. Symptomatic epilepsy, remission. High intestinal fistulas. Short bowel syndrome. Protein-energy deficiency. Cholestasis syndrome. Functional disorders of the gastrointestinal tract. Diaphragmatic hernia. Condition after surgery. Gastroesophageal reflux. Encephalopathy of mixed etilogy. |
Blood type O (I)First Rh (-) negative Kell (-) negative Phenotype (C)–(c+(D)–(E)–(e+
Anamnesis of life: a child in the neonatal period is operated on for a left-sided diaphragmatic hernia. In the n/o period frequent ARVI. In January 2016 he was hospitalized in 4 x/o. The examination revealed a relapse of a diaphragmatic hernia. 13.01.16 operation performed: Thoracoscopic plastic surgery of the left dome of the diaphragm. Was on examination in 4 x/o in October 2017. According to the examinations, moderate cardia insufficiency was detected.. Catarrhal distal esophagitis. Superficial gastritis. Confirmed gastroesophageal reflux. According to MSCT – relaxation of the right dome of the diaphragm. In 2019. the child was operated on for adhesive intestinal obstruction at the place of residence (Ct. Sochi) Laparotomy performed, adgeolisis. Real hospitalization for elective surgery.
06.04.2021 operation performed: relaparotomy, viscerolysis, fundoplication, resection of the jejunum, overlap of interintestinal anastomosis. Drainage of the abdominal cavity and small pelvis. Intraoperatively revealed a pronounced adhesion process, which required total viscerolysis.
After the operation, the child was transferred to the ICU. On admission, the condition is serious, due to the volume of surgical intervention, respiratory failure of mixed genesis (ventilation and hypoxemic), hemodynamic instability, requiring cardiotonic support. Admitted on ventilator. The stomach is not swollen, soft, painful on palpation in the area of the postoperative wound, not tense. P/o dressings are moderately impregnated with hemorrhagic discharge. Diuresis on the catheter. Urine transparent, light yellow. According to the safety drains, hemorrhagic discharge in moderate quantities.
Within 1 p/o day, independent breathing was restored, extubated. Hemodynamics stabilized. Drew attention to the pronounced pain syndrome, requiring multimodal analgesia, episodes of febrile fever up to 38,5C, drug-stopped.
07.04col. 23:00 patient's condition with negative dynamics in the form of tachycardia up to 130 / min, oppression of consciousness, on the left drainage, the discharge of the intestinal discharge was noted. Given the clinical picture of perforation of a hollow organ to a child, in agreement with Razumovsky A.Yu. and surgeons on duty, surgical intervention was performed on an emergency basis
08.04.2021: relaparotomy, resection of the jejunum, enterostomy. Intraoperatively detected perforation in 3 x jejunum sites, in 2 places these areas are resected, interintestinal anastomoses are imposed. At the level of the middle part of the jejunum, the perforation site is formed as a labial fistula in the left iliac region.
Patient returned to ICU. Given adequate spontaneous breathing, restoration of consciousness, patient extubated on morning 08.04.2021.But after 1,5 hours after extubation - an increase in DN, the child was transferred to nCPAP.Due to the increase in heart failure, vasopressor support with norepinephrine up to 0,7 μg/kg/min, followed by infusion of levosimendan (due to a decrease in the LV emission fraction to 35%), in doses up to 0,2 μg/kg/min. According to ultrasound - accumulation of fluid in the pleural cavities. In the dynamics of ultrasound - the volume of fluid without growth.
Given the significant deterioration of the condition on the background of peritonitis, intestinal paresis with translocation of bacterial flora, development of secondary ARDS, OSBS with emission fraction reduction, hemodynamic instability, condition regarded as sepsis, septic shock. Hemosorption was performed with a Cytosorb column, hemofiltration started. Due to the aggravation of respiratory failure, the patient was transferred to a ventilator. At 2p/o, taking into account the detection of carbapenemase VIM in the blood, a change of antibiotic therapy was carried out: v/v zavitsefta 62,5 mg/kg х 3p, AZNam 90mg/kg/day, decontamination-colistin 100t/IU/kg/day., metronidazole 15mg/kg/day., diflucan 12mg/kg/day., with a further increase in the dose of Zavicefta and Aznam by 30% in connection with renal replacement therapy. Repeated transfusions of erythrocyte-containing media were carried out in order to correct anemia.
By 4 p/ osotki, the condition of the child with some stabilization due to the normalization of hemodynamics, reducing doses of vasopressor support, reduction of edematous syndrome, restoration of diuresis without diuretic therapy. However,, manifestations of SPON persist (Days, Ch, Opp), fever. Against the background of A/B therapy, there is a moderate decrease in markers of inflammation (CRP 224→174 mg/l, PCT 27 ng/ml→18 ng/ml). In the blood test, a pronounced neutrophilic shift is preserved. In the neurological status against the background of opioid analgesia, there is a pronounced depression (RASS-3 points). The abdomen remains tight tense. There is an increase in hyperemia in the lower abdomen with areas of skin necrosis around the stoma. Laparotomic suture is solvent, the edges are necrotic. (Fig. 1)
In connection with the restoration of the passage through the intestine, trophic nutrition with the mixture "Peptamen" with a maximum volume of 200 was started from 4 p/o days.,0 ml/day.
But by the evening of 4 p / o day there is a discharge of intestinal contents along the left drainage. In connection with the increase in hyperemia of the anterior abdominal wall with the spread to the inner surface of the thighs and scrotum, swelling and severe soreness of this area - it was decided to carry out surgical intervention. 13.04.2021 relaparotomy performed, sanitation of the abdominal cavity - two foci are sanitized: in the pelvis and in the right, left laparostomy. (Fig. 2)
After surgery, the child's condition remained extremely serious.. The boy remained on a ventilator, continued vasopressor and inotropic support with norepinephrine up to 0,3 μg/kg/min, levosimendan 0,2 μg/kg/min. The CVVHDFc "Cytosorb" procedure was repeated. After surgery - the volume of hyperemia of the anterior abdominal wall with a significant decrease. On the laparotomic wound and stoma, the intestinal discharge departed., there was no violation of the rate of diuresis. According to the control ECHO-KG from 14.04.2021 – positive dynamics – FV with an increase to 56%. Levosimendan infusion cancelled 15.04.2021.
15.04.2021 A control MSCT study was performed - there is no data for the presence of abscesses. There is no data for perforation of the intestine to the stoma. An aspiration system made of stoma has been established, laparotomic wound. Heavy losses remain. It was decided to resume the enteral load in the amount of up to 200 ml / day with the milk mixture "Peptamen" in the probe.
Despite clinical stabilization, the child retains episodes of fever to high febrile numbers according to laboratory diagnostics, high CRP remains up to 140 mg / l, PCT rise to 32ng/ml. Given the growth of pathogenic microflora of Enterococcusfaecalis; E. coliL+hemolytic, sensitive to meroneme and co-trimoxazole, lack of data on acquired carbapenemases in the blood from 12.04.2021 - the change of antibiotic therapy to meronem drip 120 mg / kg / day and biseptol 36 mg / kg / day was performed. Change of antifungal therapy to cansidas.
In the future, an increase in the area of skin necrosis was noted., area of laparostomy. 20.04.2021 Necrectomy performed under intravenous anesthesia under ICU conditions, vacuum aspiration from the wound is established - drainage from the enterostomy and opened intestinal fistulas. A large amount of intestinal discharge departed through the aspiration system (up to 850,0 ml). (Fig. 3)
21.0On 4.2021, the child was extubated and breathed from O2-Support through high-flow nasal cannulas, Flow About2 increased to 45,0 l/min. At the moment the oxygen flow is 40,0 l/min., moderate mixed shortness of breath persists, lag of the left half of the chest when breathing. Coughs up phlegm.
22.04 In the conditions of the ICU under the AMN, necrectomy was repeatedly performed, suturing of intestinal fistulas. Drains from the abdomen and dialysis catheter were removed. With dressing 23.04 - intestinal contents flow abundantly into the wound, seam from 22.04 (intestinal fistula) is wealthy, however, a new fistula opened up next to him.. Due to the admixture of the hemorrhagic component in the intestinal discharged child, enteral nutrition was canceled.. Vacuum aspiration from the wound is constantly performed. Against the background of enteral pause and constant vacuum aspiration, the wound condition with significant positive dynamics is covered with granulations, there are no new areas of necrosis, pink fistula mucosa, Wet, Brilliant. At the moment, 4 intestinal fistulas and a labial fistula are clearly visualized., surgically applied 08.04.21.
22.04 according to MSCT and EchoCARDI - hydropericardium without signs of cardiac tamponade, in dynamics, the volume of the liquid increased. Left-sided hydrothorax was also detected and a moderate amount of fluid in the abdominal cavity is still noted.. All these signs were regarded as the course of polyserositis., 26.04 started pulse therapy with Metipred 3 mg / kg / day. In the future, according to the ultrasound of the pericardium, the fluid increased. Hemodynamics remains stable.
There is a resolution of cholestasis syndrome; remains icteric sclera, in dynamics with a decrease. Hyperbilirubinemia also with a decrease-total bilirubin of 32μmol/L, direct bilirubin (up to 16μmol/l).
Diuresis is adequate to the resulting liquid, sometimes redundant. Additional stimulation with diuretics does not require. There is no edematous syndrome. There are phenomena of protein-energy deficiency and probably, sarcopenia.
In infectious status to 17.05.2021 there is a positive trend - a decrease in markers of inflammation, leukocytosis. The child does not have a fever. In cultures from wound and abdominal cavity with 11.05.2021 multi-resistant Acinetobacterbaumanii is detected, Klebsiellapneumoniae, poly-resistant, however, given the positive clinical and laboratory dynamics, the child continues a/ b therapy with Ciplox and Metronidazole.
17.05.21. The child was transferred to the Department of Thoracic Surgery.
The condition is severe with positive dynamics. Does not feverish. The severity of the condition is due to the presence of an extensive defect in the anterior abdominal, which is gradually closing, large pathological losses on the stoma and intestinal fistulas ( 3 fistulas, 1 one side stoma). (per day approx. 940 ml. Almost complete dependence on parenteral nutrition. Breathing independently. A child in consciousness, contactee, oriented in time and space, Activated (sits and stands up on his own, walks with support). Hypotrophic. Meal (mixture 400 ml). Water 280 ml Mucous moist, Clean. Clean skin. The stomach is not swollen, moderately painful on palpation. The chair was not.
Locally: the wound is open. The surface is represented by granulations, the surface of the wound was almost equal to the skin roller. Above the stomas, a roller of mucous and granulation tissue is formed, on which the areas of epithelialization are determined. The circumference of the epithelialization zone is significantly reduced..
Conclusion: the leading surgical pathology in the severity of the condition is currently the wound process on the anterior abdominal wall, the presence of intestinal fistulas and lateral stoma, large pathological losses. It is planned to continue parenteral nutrition, conservative treatment until persistent healing of intestinal fistulas. Antibacterial therapy continue.
21.05.21. Consultation with a neurologist. The condition is severe with positive dynamics. The face is symmetrical at rest when moving. Movement of the eyeballs in full. Pupils D=S, response to light is good. Midline language. Muscle tone is symmetrically reduced, movements in the joints are possible in full. Self-attached, with the help of gets up, takes several steps. There are no meningeal symptoms. There were no seizures during the observation.
Conclusion: Condition after surgery, severe somatic condition, current purulent necrotic process with a defect in the anterior abdominal wall. Astheno-neurotic state. Epilepsy remission.
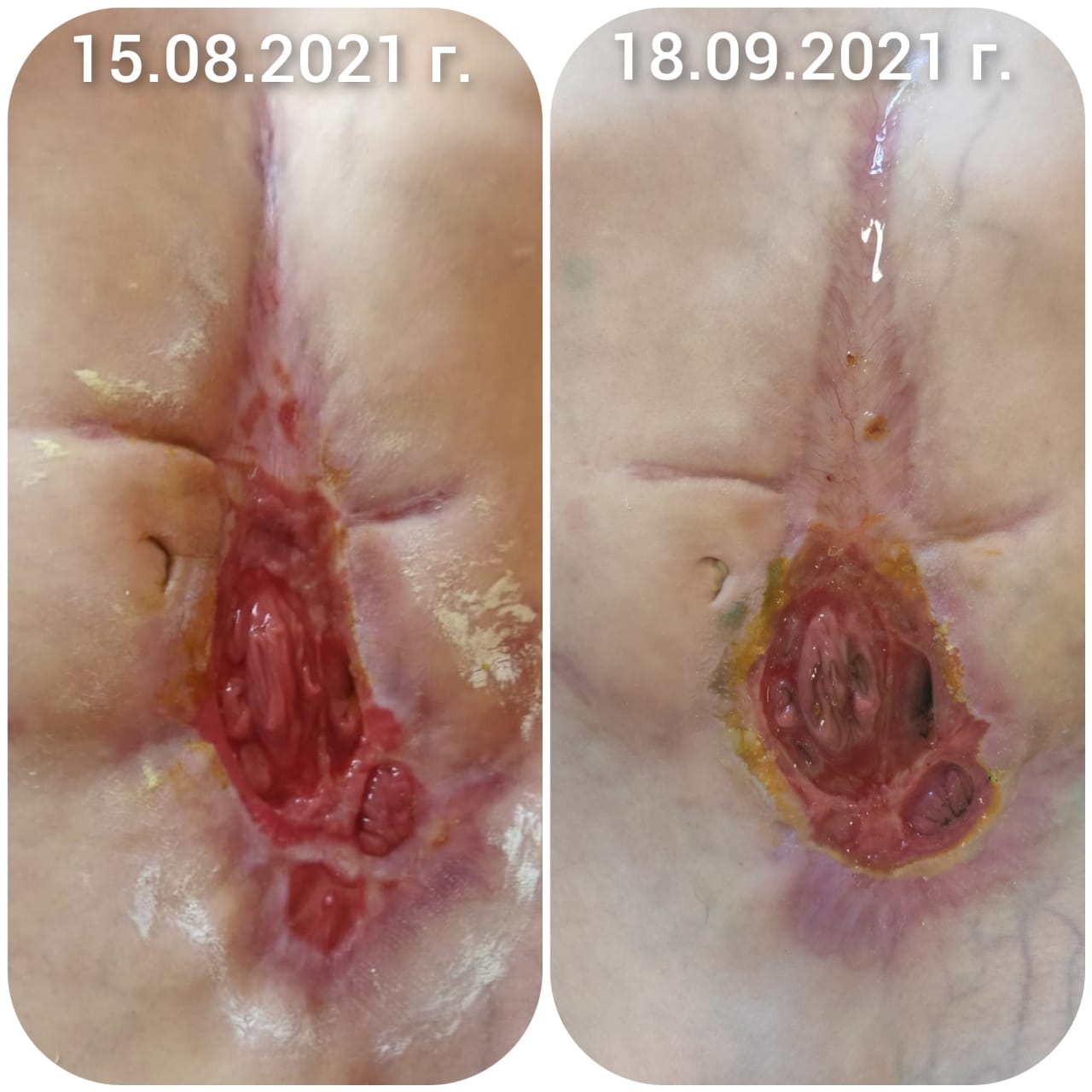
During the observation period from June to August, the condition is severe stable. The condition is severe with positive dynamics. Does not feverish. The severity of the condition is due to the presence of an extensive defect in the anterior abdominal, which is gradually closing ( large pathological losses on the stoma and intestinal fistulas ( 6 fistulas, 1 one side stoma). (per day from about 400 to 940 ml. Almost complete dependence on parenteral nutrition. Breathing independently. A child in consciousness, contactee, oriented in time and space, plaksiv, reacts negatively to inspection, interest in what is happening is reduced, Activated (sits and stands up on his own, walks with support). Hypotrophic. Meal (mixture from 50 to 400 ml). Water from 100 to 380 ml Mucous moist, Clean. Clean skin, periodically there is ectericity of the skin sclera and skin. The stomach is not swollen, moderately painful on palpation. Stool in scanty quantities rarely (1 time per week) there has been no stool in the last two months. What is associated with the separation of the stoma by the edges of the epithelializing wound. (Fig. 5)
17.09.21. For a month, the wound was treated with ZHKM by gradually defrosting 100 ml of the container and applying to the entire surface of the wound during the day.. During observation, the state with some positive dynamics, in consciousness, communicates with others, performs school assignments. Periodically subfebrile fever. Enteral load in the form of a mixture Modulin does not fully absorb 50-500 ml per day. Periodically there is nausea and vomiting. Meat and vegetable puree 20-30 ml per day, soldered with saline and water. The severity of the condition is due to the presence of high intestinal fistulas on the anterior abdominal wall with large pathological losses on the stoma and intestinal fistula. (per day about 500 -1000 ml). Hypotrophy, protein-energy deficiency. Thrombosis of the right femoral and iliac vein. Almost complete dependence on parenteral nutrition (kabiven). Breathing independently. Dry mucous membranes. Clean skin. The stomach is not swollen, moderately painful on palpation. There was no chair for 2 months.. Saline solution is injected daily into the eyonostomy, glucose, petroleum jelly, probiotics. Physical activity does not tolerate well, quickly depleted, can move without support.
Locally: the upper part of the wound is almost closed. the width and length in the upper sections is significantly reduced and is represented by scar tissue. . In the lower part of the wound and in the middle third, previously formed pockets, Closed. In the lower part of the wound is a jejunostoma, on which the intestinal discharge departs. 6 fistulas formed on the surface, two of which are of the "double-barreled" type. The diameter of the wound is currently 6,0 see. caloric receiver installed. (Fig. 6 )
In the future, the child is repeatedly operated on., as a result, the laporostomy and intestinal fistulas were closed and the passage through the intestine was restored. The child was discharged home in a stable condition.
Conclusion on the use of LCD: observation of the course of the wound process in the laporostomy shows an acceleration of granulation and epithelialization of the edges of the wound and a reduction in the wound area.




 Loading...
Loading...